Cardiac rehabilitation is a program to help patients with heart events recover and return to normal activities. It is recommended following acute heart events and as a component of addressing chronic heart failure. Despite recommendations from federal agencies, advocacy groups, and national health associations and the documented benefits of cardiac rehabilitation, only 20-30% of people who could benefit from it actually attend cardiac rehab. Million Hearts, an initiative cofounded by the Centers for Disease Control and Prevention (CDC) and Centers for Medicare and Medicaid Services (CMS), has set increasing the use of cardiac rehab as one of its priorities. By 2027, they hope that at least 70% of people for whom cardiac rehabilitation would be appropriate will participate.
Using HCCI’s data on people who get insurance through work and CMS data on the Medicare and Medicaid populations, we highlight trends in cardiac rehabilitation. We look at the rate of cardiac rehabilitation sessions relative to the rate of acute heart events, which allows us to see differences between groups and overall trends in cardiac rehabilitation rates by accounting for the underlying rate of heart events.
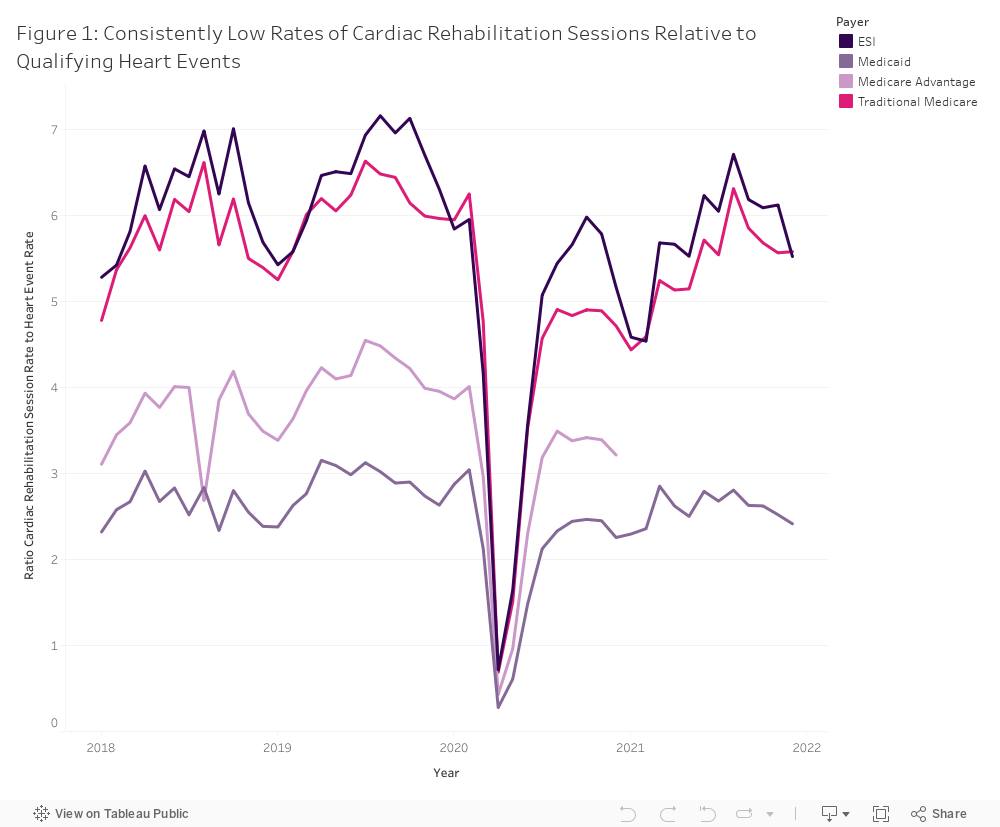
In 2021, across all populations, the data show that people with qualifying heart events are not accessing cardiac rehabilitation at recommended rates. A standard cardiac rehabilitation program typically includes 36 sessions over 12 weeks or approximately 12 session per month. Among people with Medicare and employer-sponsored insurance (ESI), the average cardiac rehab visit per qualifying event was less than half that. People enrolled in Traditional Medicare averaged 5.4 cardiac rehabilitation sessions per cardiac event in a month. Among people with ESI, the monthly average was 5.7 per event. In Medicaid, the rate of cardiac rehabilitation to acute heart events was less than a quarter of the standard – only 2.5 sessions per qualifying event.
Figure 1 also shows that cardiac rehabilitation rates dropped by about 25% in 2020 compared to 2019 across all payers. Although rates rebounded from 2020 to 2021, they remained about 10% lower than they were in 2019 across all payers. Several factors could play into this decrease. Other research identified about 8% of cardiac rehab services that served Medicare beneficiaries closed during the pandemic, which was not offset by the number of new cardiac rehab centers that opened during the same time nor by the availability of telehealth waivers for virtual sessions among Medicare beneficiaries. That same paper found that closed facilities primarily served rural, low income and socially vulnerable communities.
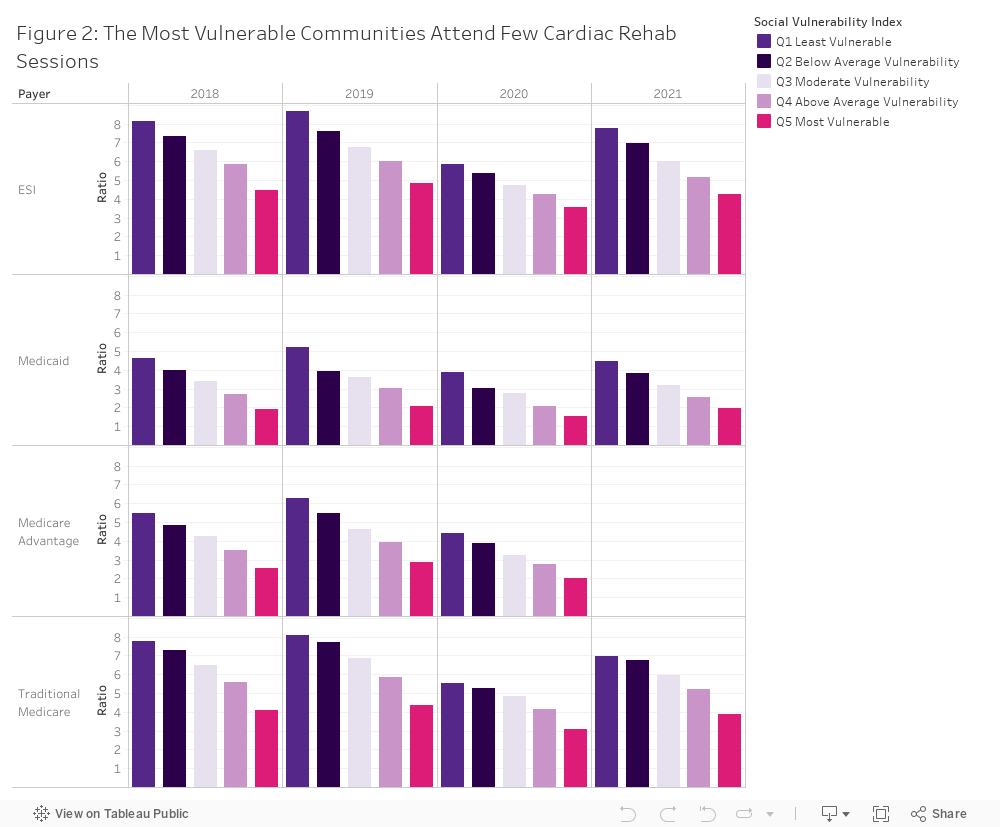
Focusing in on 2019, we observe a wide gap in rate of cardiac rehabilitation session attendance relative to qualifying heart events by SVI quintile across all payers. The ratio of cardiac rehab relative to qualifying events in the most vulnerable communities is about half that of the least vulnerable communities. While the ratios between groups varied during the pandemic years, the relative disparities continued to exist. Lack of equitable access to cardiac rehab is well documented, with research indicating that rural, low SES areas and other underserved populations have lower participation rates in cardiac rehab programs.
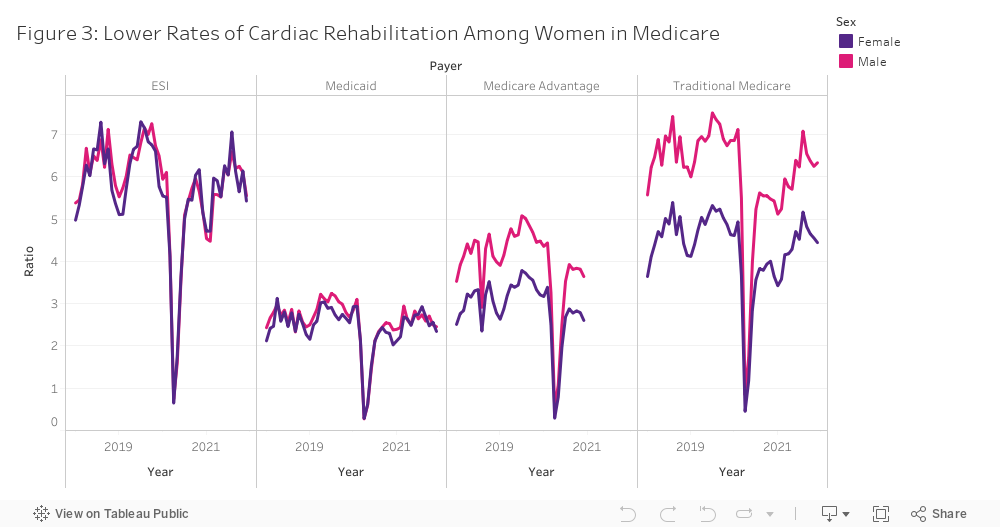
Among people enrolled in ESI and Medicaid, cardiac rehab rates were similar between men and women. However, on average, women enrolled in Medicare had 30% fewer cardiac rehab sessions (4.4 female vs. 6.1 male); this held true among both Medicare Advantage and Medicare FFS enrollees.
This report is consistent with other analyses that show low use of cardiac rehabilitation, especially in the most vulnerable communities, among women, and with advancing age. Future work can continue to explore the relationship between patient characteristics, social factors, and other barriers to access and use of cardiac rehabilitation programs.
More data on cardiac rehabilitation and qualifying heart events can be found in the Health Care Vitals Dashboard on HCCI’s website.
Methods
We used HCCI’s unique employer sponsored insurance claims dataset, Medicare Fee for Service claims, Medicare Advantage Encounter records and Medicaid TMSIS files to examine the rate of cardiac rehab sessions relative to the rate of acute heart events (Acute myocardial infarction (AMI), Coronary artery bypass graft (CABG) surgery, Heart valve repair or replacement procedure, Percutaneous coronary intervention (PCI; includes percutaneous transluminal coronary angioplasty [PTCA] or coronary stenting and same-day discharge after an outpatient PCI), Heart or heart-lung transplant). This metric allows us to see differences between groups and overall trends in cardiac rehabilitation rates by accounting for the underlying rate of heart events.
We adapted rates from the Million Hearts Cardiac Rehabilitation Use Surveillance Methodology. We first identified outpatient cardiac rehabilitation claims as well as claims with diagnoses or procedures for Acute myocardial infarction (AMI), Coronary artery bypass graft (CABG) surgery, Heart valve repair or replacement procedure, Percutaneous coronary intervention (PCI; includes percutaneous transluminal coronary angioplasty [PTCA] or coronary stenting and same-day discharge after an outpatient PCI), Heart or heart-lung transplant from 2018 to 2021. These Cardiac rehabilitation rates were calculated as the total number of cardiac rehab sessions per 100,000 enrollees (i.e., the rate includes those who did not utilize any cardiac rehabilitation services). Cardiac event rates were calculated as the total number of unique patients with a heart event per 100,000 enrollees. We used these two rates to calculate the average rate of rehabilitation sessions per unique heart event.
All enrollees with known age and sex were included in the denominator. The ESI and Medicaid populations were limited to those between the ages of 25 and 65, the Traditional Medicare and Medicare Advantage populations were limited to enrollees over the age of 25. Some states were excluded from Medicaid analysis due to data quality issues.